10 Year Study Proves Better Option for Repair of Unstable Distal Clavicle Fractures

New York, NY (PRWEB) August 03, 2016 -- Dr. Steven Struhl, a leading Orthopedic Shoulder Specialist, announces the publication of his 10-year study in The American Journal of Sports Medicine. The study reveals that his "Closed-Loop Double Endobutton" technique has better results to repair an acute unstable distal clavicle fracture than other procedures that requires either additional surgery to remove hardware or potential complications from knot slippage. Following the in-depth study of 35 patients of Steven Struhl, MD (Orthopedic Surgeon and Shoulder Specialist) where he performed his patented "Closed-Loop Double Endobutton Repair" procedure for an Acromioclavicular Joint Separation, Dr. Struhl realized that the same breakthrough procedure could be applied to an unstable distal clavicle fracture.
Figures show that there are approximately 200,000 cases of clavicle fractures that occur each year in the U.S. Although a good percentage of those can be managed non-surgically, a specific type, Neer type 2B fracture, poses a more challenging problem. The Neer IIB injury comprises a fracture between the coracoclavicular (CC) ligaments with complete rupture of the conoid ligament.
Other methods achieve fracture union, but morbidity varies widely
Recent studies do find that traditional techniques of either a direct osteosynthesis with plate or indirect stabilization of the CC interval with suture, screw, or cable fixation does achieve fracture union 97% to 100% of the time, however morbidity varies widely between techniques.
• Direct osteosynthesis with standard plating techniques are challenging and often impossible due to distal fragment size and/or comminution. Additional surgery is usually required, since plate removal is required 40% to 53% of the cases.
• Even though the traditional indirect techniques relying on CC stabilization does not require a second operation to remove hardware; knot slippage and abrasion could potentially occur.
Suture-Button configuration prone to knot slippage and abrasion
Previous studies have shown that suture-button configurations that require a knot have poor results as a long-term solution. In fact, studies have shown that this method experiences slippage in 31% to 50% of the cases, as well as surgical complication rates of 27% to 52%.
New technique for fixation reduces knot slippage
Dr. Steven Struhl and his team realized that the successful outcomes of his Continuous-loop Double Endobutton technique that was designed to address issues of slippage and proved to be consistently successful for an AC Joint separation could easily be applied for a distal clavicle. With his success and in-depth study with 35 patients over 11 years using his breakthrough technique to repair AC Joint Separations, Dr. Struhl, being a true visionary, knew that this modern procedure could be used effectively for acute Neer type IIB distal clavicle fractures.
U.S. Patented "Closed-Loop Double Endobutton Repair" or "Continuous Loop" for Neer Type 2B Distal Clavicle Procedure with superior results
This study demonstrated that the use of a continuous loop design, significantly improved outcomes over standard suture-button configurations. Results proved that the “closed-loop” eliminates the problem of knot slippage or breakage that is inherent to a standard suture-button device. More importantly the loop has similar stiffness and more than double the strength of one’s own ligament. The "loop" was found to be durable and reliable, showed effective healing, and additional surgeries were avoided.
Patented Technique
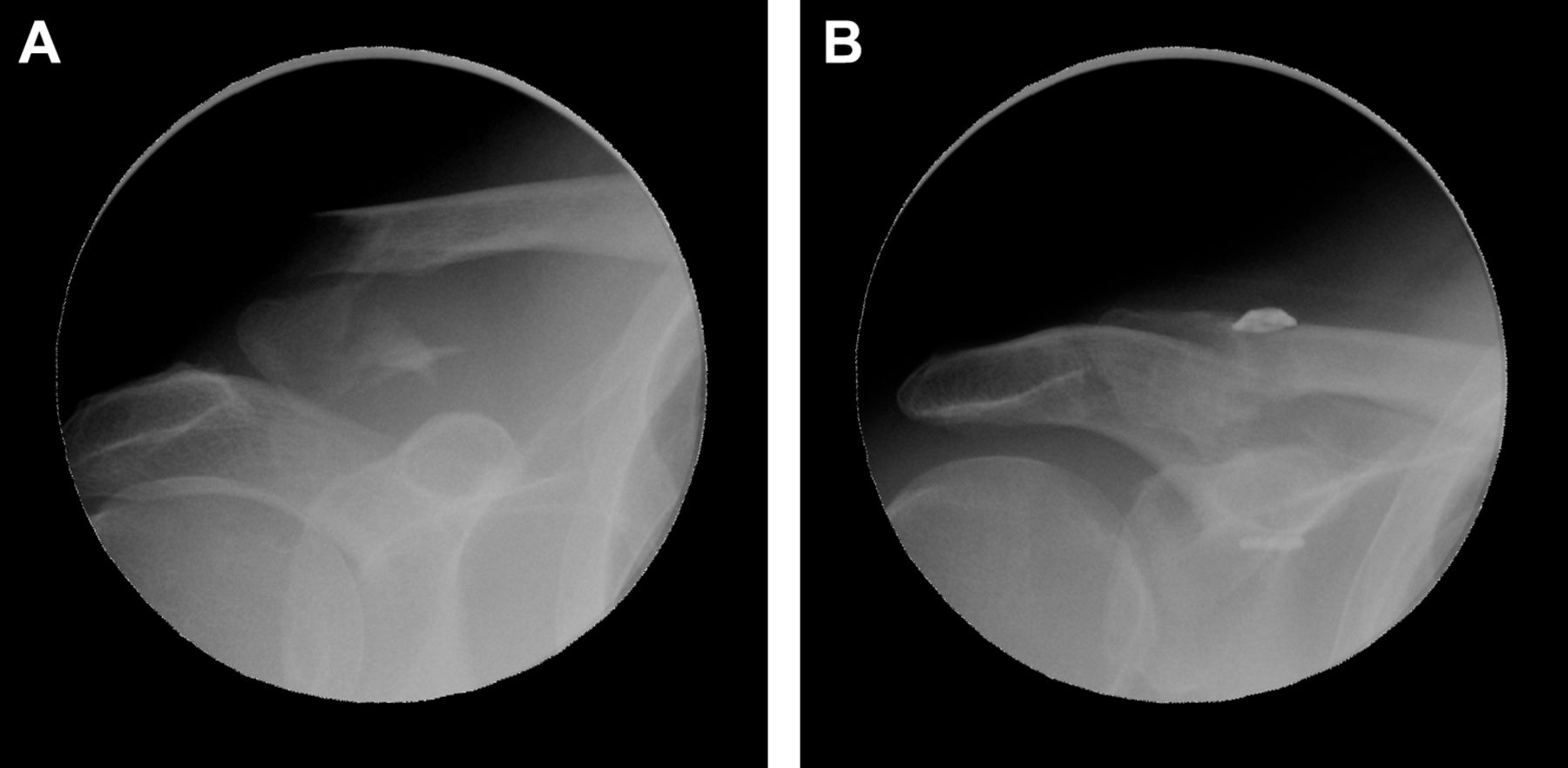
Dr. Struhl explains, “The surgical design was to use a continuous loop to eliminate knot breakage and slippage, is in line with biomechanical principles and always creates a biologic connection between the coracoid and the clavicle. The technique is open, the joint is reduced, a hole is drilled, the channel length is measured and the appropriate loop size is chosen and prepared with sutures. When the measured channel is within 1mm, a standard endobutton is used. When the measurement is in between, a larger loop is chosen, which leaves excess loop that is filled with an extended button that is thicker and wider and compensates for the extra loop.”
Study Group with comprehensive evaluations
The study group consisted of 8 patients, who were followed for 1 to 9 years. Industry best practices of outcome scoring systems were used to validate results. Follow-up information was obtained on all 6 of the 8 patients, since 2 were unreachable and lost to follow-up. The 6 patients underwent a detailed functional and radiologic evaluation.
The Results
Across the board positive scores!
At follow up, the average mean raw constant score was 97 and normalized constant score of 99 (0-100), the mean University of California, Los Angeles Shoulder Rating Scale score was 33 (0-35), the mean American Shoulder and Elbow Surgeons Shoulder Score (ASES) was 98 (0-100) and the Simple Shoulder Test (SST) score was 11.2 (0-12).
At a minimum 1-year follow-up, all patients had achieved radiographic union. There were no cases of non-union or osteolysis. One patient had temporary wound breakdown, which resolved with local wound care. No surgical site infections or perioperative fractures were observed. No patients complained of hardware irritation or prominence. There were no cases of reoperation or revisions.
Why does the Double Endobutton Continuous Loop Work?
• It has a strong and durable fixation
• Allows for normal physiologic movement
• Surgeon friendly that minimizes complication risk and plan for long-term biologic stability.
About Steven Struhl, MD
Steven Struhl, MD is board certified in both Orthopedic Surgery and Sports Medicine/Arthroscopic Surgery,and has been in private practice for over 23 years. He is currently on faculty at NYU Langone Medical School and is a member of the teaching service at the Hospital for Joint Diseases. He has authored numerous peer review articles and his research has been presented both nationally and internationally.
For more information about Dr. Steven Struhl’s patented “Closed-Loop Double Endobutton Repair” for Neer type IIB distal clavicle fracture, please visit http://www.shouldersandknees.com. For a copy of this study, please visit http://ojs.sagepub.com/content/4/7/2325967116657810.full
Steven Struhl, MD, Steven Struhl, MD, http://www.shouldersandknees.com/, +1 (212) 207-1990, [email protected]
Share this article